

Repost: Approaching risk, objectives, and interventions
Repost: Approaching risk, objectives, and interventions

In Frameworks and Essentials for optimizing health and Longevity, I describe how longevity consists of lifespan and healthspan, i.e. how long and well we live.
Improving longevity comes first and foremost down to delaying the onset of chronic disease. There’s a very predictable set of diseases that will plague the vast majority of people as they age. Aligning objectives with the best knowledge of prevention is the basis for developing strategies combating the inevitable decline.
Only after defining objectives, in high resolution and very concretely, does the challenge become approachable. Although embracing the arc of life and accepting the age-related physical decline is part of the emotional flexibility that allows a sense of peace with the inevitable, so is taking responsibility for one’s own health.
A measure of healthspan often used in epidemiology and public health is the so-called Disability-adjusted life years (DALYs). The world health organization rationalizes and defines DALYs in the following way: “Mortality does not give a complete picture of the burden of disease borne by individuals in different populations. The overall burden of disease is assessed using the disability-adjusted life year, a time-based measure that combines years of life lost due to premature mortality and years of life lost due to time lived in states of less than full health, or years of healthy life lost due to disability. One DALY represents the loss of the equivalent of one year of full health.”
The concept of DALYs is the first step towards quantifying healthspan, but leaves room for improvement. Being free of disability and disease as an objective is vague and barely useful. Instead, taking a pragmatic, concrete, and actionable approach via backcasting to define our objectives will yield us the highest probability of reaching desired outcomes.
Backcasting involves envisioning a desirable future, discounting, and deciding an appropriate level of performance in the present, given the rate of inevitable decline. This removes a significant amount of stochasticity compared to approaches focusing on improvement in the short-term and allows for more flexibility in the long run. Backcasting includes envisioning alternative outcomes and preparing for these accordingly, which is essential due to the partially random nature of life.
Backcasting is also a tool for accountability. Defining the future for oneself necessitates present levels of performance to keep up with at least the rate of decline while quantifying the current yields valuable insight on the effectiveness of interventions taken to achieve sed future.
The more concrete the goals the better. Being more precise and granular than “being free of disability and disease” or “able to do the activities of daily living” will increase the probability of success and help keep a tight focus on the objectives. Being able to walk a golden retriever for 30 minutes at a decent pace, twice a day, in hilly terrain, in any weather, is the level of precision that allows deliberate tactics.
Delaying the onset of chronic disease is the overarching, probabilistically strongest approach to longevity. Essential to this approach is premortems. Premortems involve envisioning undesirable outcomes and using backcasting to figure out what necessary and/or sufficient conditions had to be true for the outcomes to occur.
Avoidable conditions [in the broad sense of the word, not disease] are then to avoided by means of satisfying frameworks for interventions, while unavoidable conditions should be hedged against.
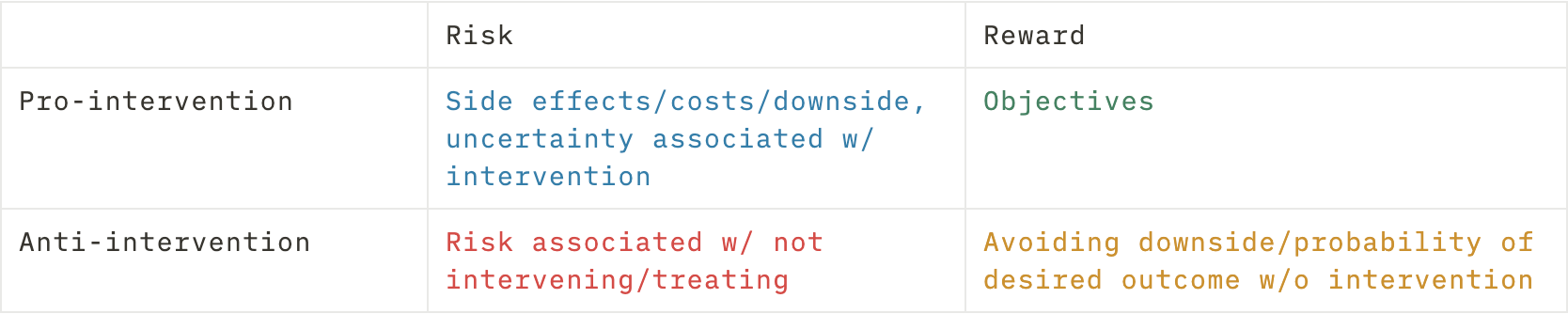
An intervention is defined as “a measure taken to prevent or treat disease or to improve health in other ways.” Inherent to all interventions are opportunity cost and downside risk. Effective resource allocation becomes crucial due to time, energy, financial, and preferential and social constraints. Deciding which interventions to approach minimally and which to go all-in on should be predicated on risk assessment, objectives, and personal uncertainty tolerance, as the evidence of the effectiveness of different interventions varies.
Conceptualizing risk, expected outcome, and variance associated with interventions require rigorous analysis of the effectiveness and downsides of the interventions. Of equal importance is the analysis of the contra-negative, i.e. the risks associated with not intervening.
Tools for assessing risk yield valuable and actionable insights if used correctly and under the proper scrutiny. Modalities like family history, biomarkers, imaging, disease-specific tests, body composition, living environment, and so on, offer often varying but useful insights depending on the condition of concern.
Understanding what information different modalities can and cannot yield, and interpreting the information in the broader context of health becomes essential when deciding on interventions and strategies. Modalities used for receiving feedback and tracking progress on certain metrics should not be confused to represent overall or general health.
Stacking tools for obtaining the most wholesome picture sets us up for the highest probability of achieving our objectives with the least risk of anything flying under the radar.
The process then becomes predicated on subjective objectives, risk tolerance, and “time in the market”. Financial metaphors fit in very well to describe the importance of acting early. Starting to save for retirement in one’s ’50s vs. 20s requires setting aside a lot larger amounts, taking on more risk, and ultimately enduring larger volatility and lower probability of pay-off while compromising more in the immediate to short term.
The same holds for the benefits of exercise, sleep, nutrition, and emotional health. With time and age establishing changes and habits become harder due to the inevitable decline of physical performance and stature, reduced plasticity and emotional flexibility, and the increasing amounts of responsibility not allowing excess risk-taking or devotion of time.
The so-called five tactics of the longevity toolkit; nutrition, exercise, sleep, mental and emotional health, and pharmacology and supplements, are the dimensions across which interventions are deployed. Objectives are attained and set up by the processes of backcasting and using premortems, considering previously mentioned modalities like family history and biomarkers, the state of current affairs, and a vision of years and decades to follow. Crafting a tailor-made approach that aligns with subjective values and objectives will be the way forward.
The practitioner’s role in this process is, first of all, to set up the strategy, but more importantly to monitor and adjust. Working out at the practical level what works for each and everyone in a multivariable environment requires specific knowledge and an unbiased perspective. Self-evaluation and adjustment work somewhat, but personal biases can result in undesirable directions and taking on excess burden. The five tactics are tightly linked to identity and self-perception, and it’s not unusual for these things to either be hard to tackle and change, or to become overly rigid and obsessive around required practices. A practitioner steeped in these approaches can help to evaluate not only the measurable impact brought about by the tactics but also the more human aspects of the journey towards a longer and more fulfilling life.